USABILITY TESTINGExperience of obtaining medication (initiation)
FINDING #1
Lack of guidance on how to manage medications
Of 22 participants, over half (13) used trial and error to find their current adherence strategy; 5 participants used previous experience of helping someone else manage their medication and 4 received suggestions from a friend or family member. No participants received guidance from a medical professional about how to devise an effective medication management practice, such as where to put, how to store, or how to develop a routine around taking their prescription medications.
Implication: This lack of guidance from medical professionals presents a missed opportunity to increase medication adherence, especially with the low adherence rate in the US.
FINDING #2
Increasing mail orders and 90-day supplies
Two thirds of participants had prescriptions delivered by mail and almost all [21/22] received a 90-day supply of medication.
Implication: Mail order further limits opportunities for pharmacist guidance, such as how to correctly take medications, or patients to ask questions. This is further compounded by almost all participants receiving a 90-day supply.
Experience taking medication at home (implementation)
FINDING #1
Great variance in medication management
No two participants had a medication management routine that was exactly the same. This was despite some participants using similar adherence devices or taking medication at similar times. For participants who used a pill case, there was great variety in when they refilled their pill case; where they stored their pill case; and how they remembered to take their medication. For other participants, they developed unique, complex routines that included tactile triggers. One participant flipped her pill bottles and moved it across the microwave to keep track of their adherence.
Implication: Medication management is complex and is developed to fit a unique daily routine and person. What works for one person may not work well for another.
"I came up with a scheme, where I keep the medicines on one side of my microwave, or my toaster oven. When I take it, I put it on the other side."
– Participant 4
FINDING #2
Pill case was the most popular adherence device
Majority of participants[17/22] used a pill case.
Implication: Weekly pill cases may be popular because they provide direct feedback on whether or not someone took their medication using visual cues.
.png)
FINDING #2
Reliance on multiple triggers to remember to take medications
For this study, we define adherence triggers as actions that are taken or objects that are encountered that help patients remember to take their medication. All (100%) participants relied on at least two triggers to remind them to take their medication, while 68% relied on three or more. Action triggers included eating a meal (50%) and getting ready for bed (25%); object triggers included a pill case (77%) and a water glass (18%). One participant who relied on three triggers – taking medication with a meal, using a pill case, and placing it on the dining table – missed the first trigger but saw their pill case which acted as a fall back reminder.
Implication: Under some circumstances, multiple triggers served as “a safety net,” providing different avenues for medication reminders. How can we leverage this to improve adherence routines?
Underlying reasons for non-adherent behavior (persistence)
FINDING #1
Change of routine was the greatest contributor to non-adherence
The most common reason for non-adherence among participants was a change of routine[13/22], which caused an absence of a specific trigger. For example, one participant who relies on breakfast as a trigger forgets to take her medication when she skips breakfast:
Implication: Implication: How can we make an adherence strategy durable under a change in daily routine?
"If I have to go somewhere, first thing in the morning, that's a typical time when I forget. Because sometimes I don't even have time for breakfast or for one reason or another didn't get around to it. Then the next day, it's Monday, but I'm looking at the Sunday case saying, ‘Oh, I guess I forgot to take it yesterday.’ " –Participant 7
Conclusions
All participants in our study did not receive guidance from a healthcare professional about how to manage their medication or develop an adherence strategy. Given that we know many patients struggle with adherence, there may be value in guiding patients to develop an effective adherence strategy or recommend changes to make their current strategy stronger. Secondly, people develop unique – and sometimes surprisingly complex – routines to remember to take medication. For example, participants relied on multiple action and object triggers to remember to take their medication. Participants also became less adherent during the absence of usual triggers such as a change of routine. We hope to further probe what makes a trigger durable under disruptions to routines; if multiple, durable triggers lead to greater adherence; and how to guide older adults in developing a more successful medication strategy. Lastly, time-based reminders are the most common reminder mechanism in consumer medication management apps and devices, but few study participants reported using them or taking their medication at an exact time, instead relying on routines and time ranges. Medication nonadherence is a growing problem, which reminders can potentially mitigate. Our results highlight the need for research outside of time-based reminders, such as routine-based reminders, to increase medication adherence. While a small sample, the analysis suggests that there are opportunities to provide guidance to older adults in developing an adherence strategy and design better aids to adherence that leverage established daily routines.
Co-design activities
We had two co-design activities. The first revolved around understanding the overall patient experience from being prescribed a medication to adhering to their medication and identifying pain points along the way. The second focused on blue sky ideations about possible solutions addressing those pain points.

Activity 1: User Journey Map & Pain Points

Activity 2: Blue sky ideations
Pilot Evaluations
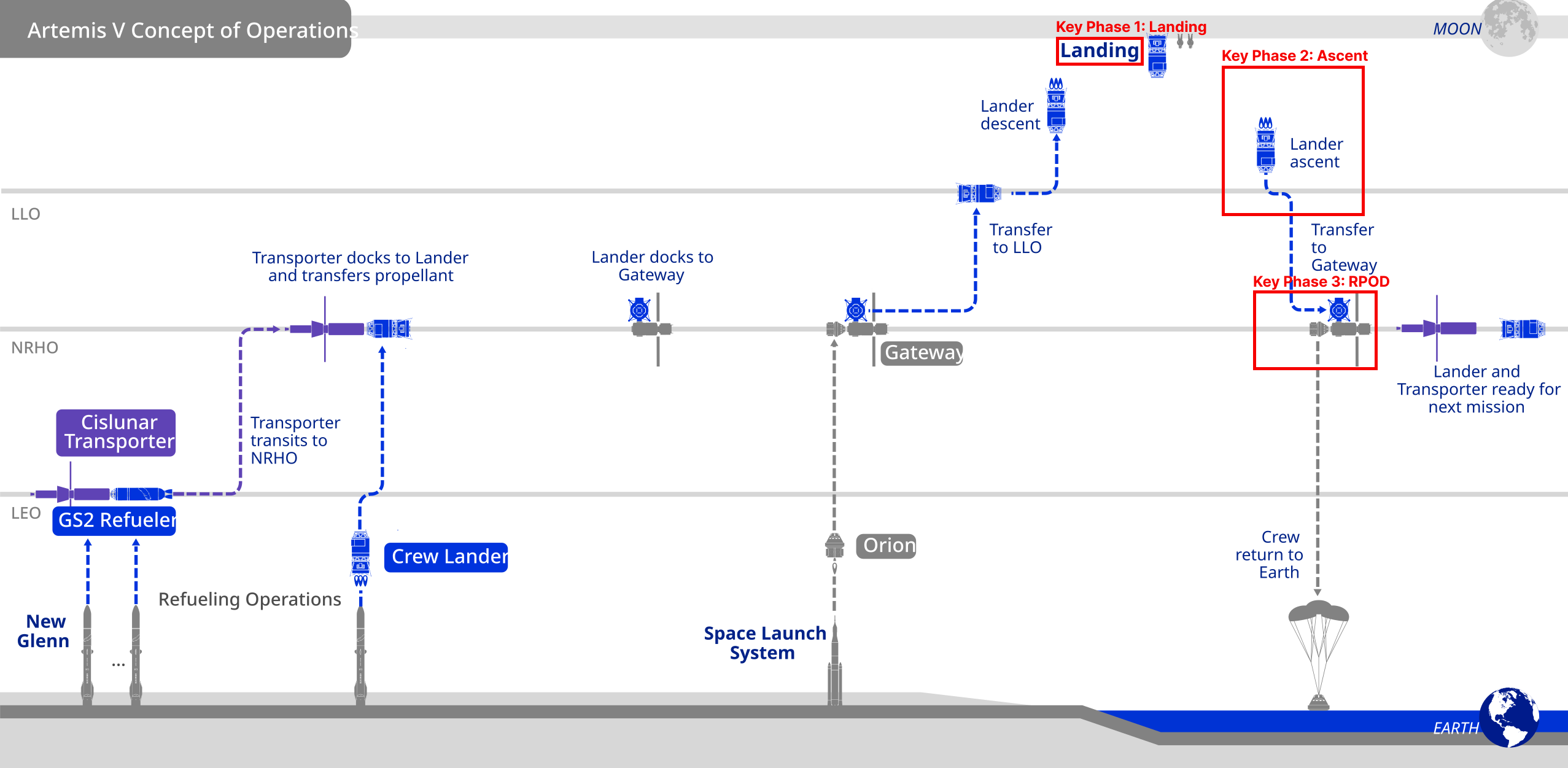
How did I test my designs?
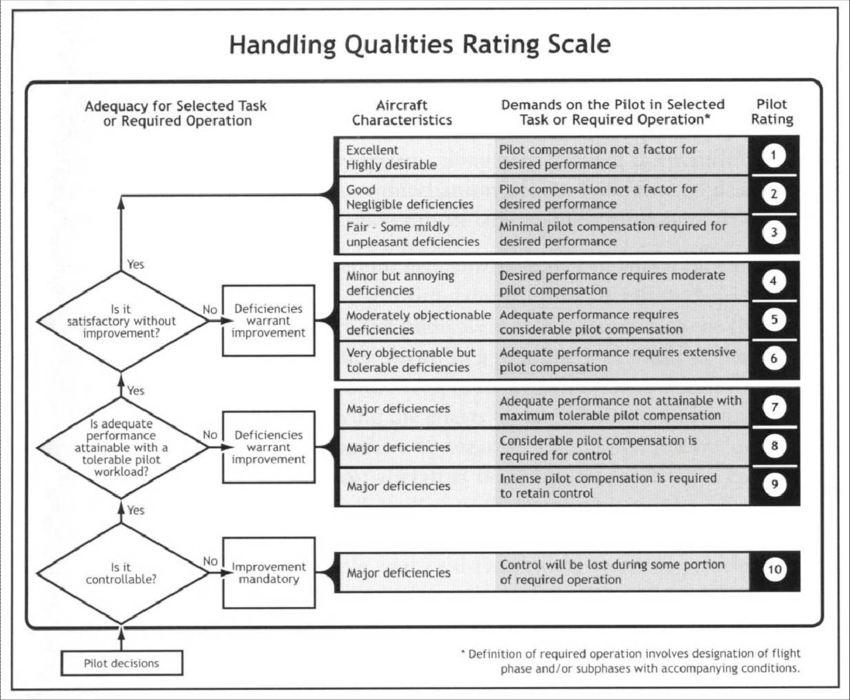
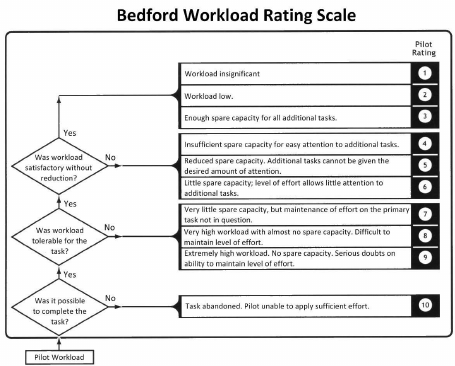
Pilot evaluations took place in the span of 4 days. I helped run testing for landing, ascent, and RPOD in the lab by moderating and taking notes. Test pilots were debriefed/ trained beforehand. I collected data on workload using the Bedford workload scale and handling qualities using the Cooper-Harper Rating Scale after each run. After a pilot went through all their runs for a phase (landing, ascent, or landing), I helped conduct a debrief interview.

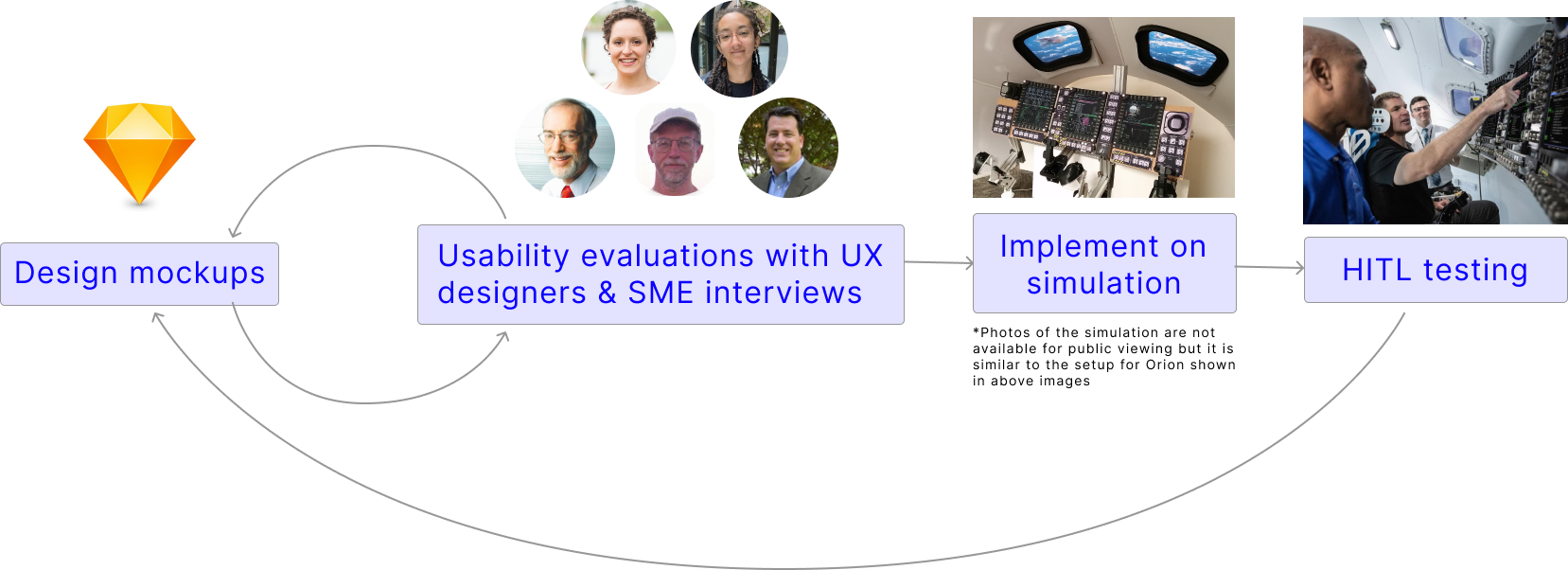
image of Orion cockpit simulation setup
HITL Simulation Setup
○ The simulation setup is not available for public viewing but it was similar to the Orion cockpit w/ windows, display panels, and hand controllers
○ Test pilots wore eye tracking glasses
Measuring Handling Qualities
○ We used the Cooper-Harper Rating Scale to measure vehicle handling qualities after each simulation run
Measuring Pilot Workload
○ We used the Bedford Workload Scale to measure pilot workload after each simulation run
Ascent Presentation to Test Pilot Team
○ After the test pilot team completed their ascent runs, I presented and facilitated a discussion on the long term ascent designs. I received feedback on my designs, which informed my next design iteration.

Me and my colleague in the Draper atrium
Handling Qualities Report & Design Iteration
How did I synthesize and take action on results from Pilot Evaluation?
Handling Qualities Report
I synthesized qualitative and quantitative findings for ascent and created a list of design recommendations for our next design iteration. My analysis was included in a Handling Qualities report that was given to Blue.
Design Iteration
I mocked-up potential design changes based on the handling qualities report. I also created an ascent handoff documentation describing each design component, rationale for the component, and a traceback to a HITL or SME interview that justified my design decisions.
.svg)





.png)